A blood clot in lungs usually refers to a pulmonary embolism, often shortened to PE. This happens when a clot, most commonly one that formed in a deep vein in the leg, breaks loose, travels through the bloodstream, and blocks blood flow in the lungs. It is not just a “breathing problem.” It can quickly strain the heart, lower oxygen levels, damage lung tissue, and become life-threatening if treatment is delayed.
What makes this topic so important in daily life is that the people at risk are not limited to one narrow group. A blood clot in lungs can happen after surgery, during cancer treatment, after long periods of immobility, during or after pregnancy, or in someone with a prior history of clotting problems. It can also happen in people who did not realize they were developing a clot in the first place.
The symptoms can be dramatic, like sudden shortness of breath, sharp chest pain, coughing up blood, or fainting. But sometimes the warning signs are more subtle at first. Some people have mild breathlessness that worsens over hours or days. Others have no obvious leg symptoms beforehand, which is one reason pulmonary embolism can be missed if people assume it is just anxiety, muscle strain, or exhaustion.
This guide explains what a blood clot in lungs actually is, the different ways it may show up, why it happens, what raises the risk, how doctors diagnose it, what treatment and recovery often involve, and what practical steps may help reduce the chance of another clot. This article is for education only and is not a substitute for urgent medical care, diagnosis, or treatment. If someone has sudden breathing trouble, chest pain, fainting, or coughing up blood, emergency evaluation is appropriate.
Table Of Contents
- Understanding blood clot in lungs
- Types Of blood clot in lungs
- Causes Of blood clot in lungs
- Symptoms Of blood clot in lungs
- Risk Factors
- Diagnosis Process
- Living With blood clot in lungs
- Prevention Strategies
- Practical Examples
- Conclusion
- Frequently Asked Questions
- Final Editorial Disclaimer
- References
Understanding blood clot in lungs
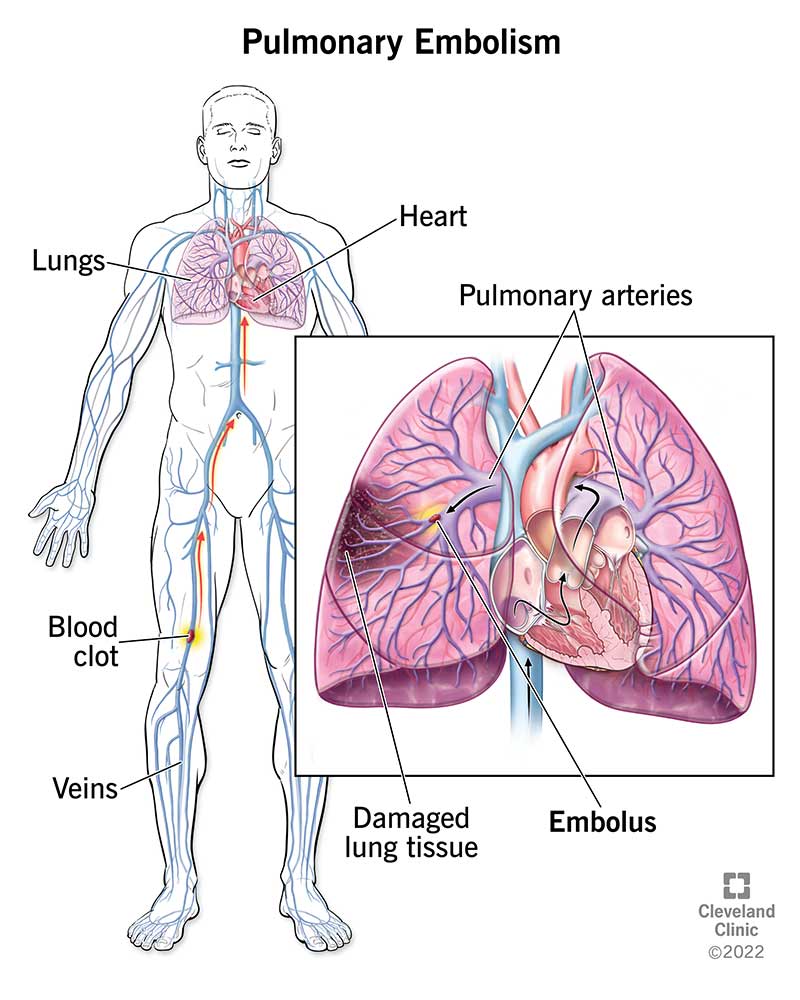
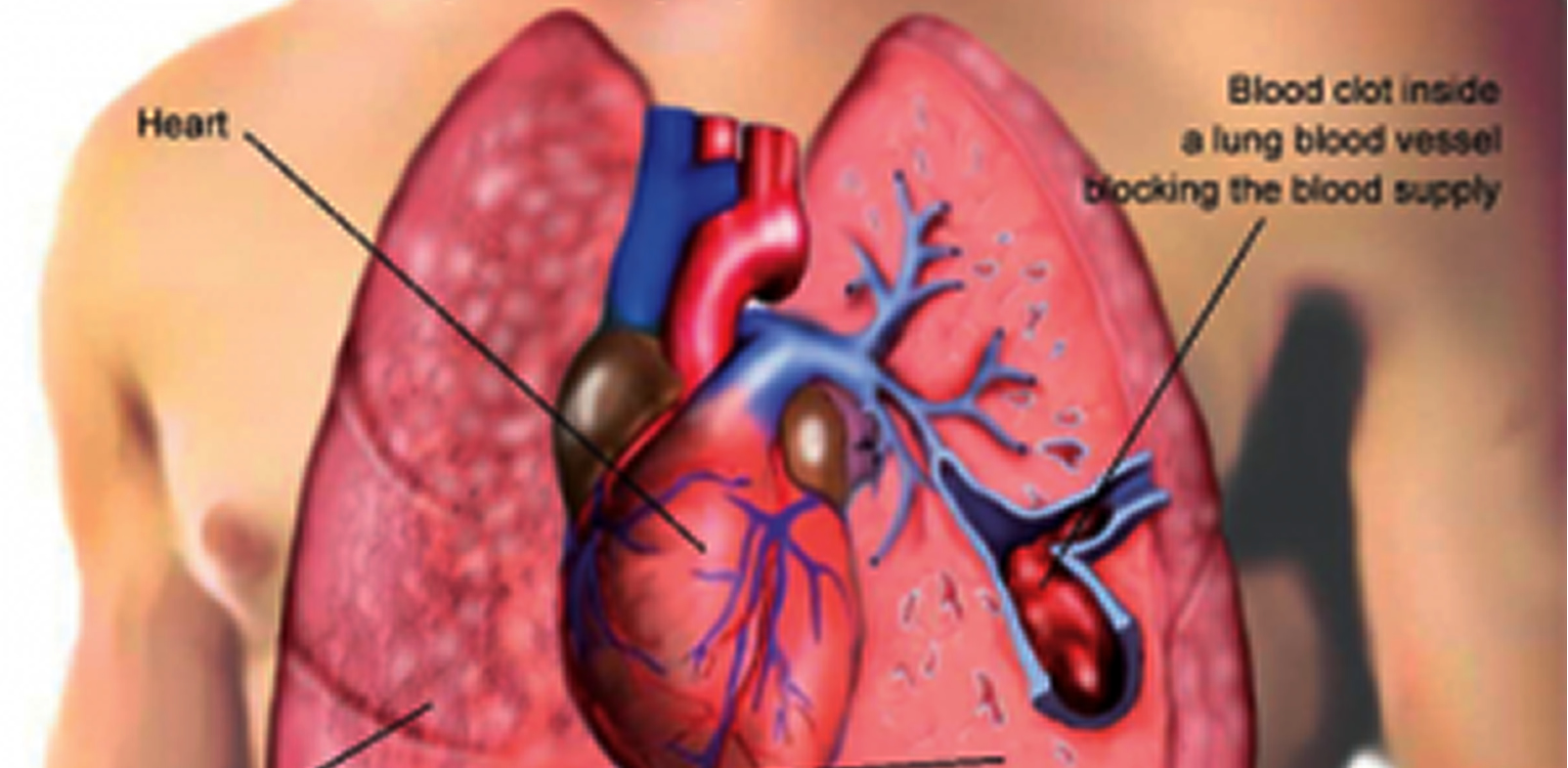
A blood clot in lungs is usually a pulmonary embolism. In plain language, it means a blood vessel in the lung gets blocked by a clot. Most of the time, that clot did not begin in the lung. It started elsewhere, usually in the deep veins of the leg, where it formed quietly as a deep vein thrombosis, or DVT. Then part or all of that clot traveled through the right side of the heart into the lungs.
To understand why this matters, it helps to picture the lungs as more than air sacs. They are also a huge network of blood vessels. Every breath you take only works if blood can flow through the lungs, pick up oxygen, and carry it to the rest of the body. When a clot blocks that flow, the body can suddenly struggle to oxygenate properly. The heart, especially the right side, may have to pump much harder against the blockage. That is why a pulmonary embolism can affect breathing, circulation, stamina, and survival all at once.
Another important point is that the phrase “blood clot in lungs” sounds like a single fixed condition, but real cases vary a lot. A very small clot may cause mild symptoms or none at all. A larger clot can cause intense shortness of breath, low blood pressure, collapse, or even sudden death. More than one clot may be present at the same time. The size, location, and the person’s overall heart and lung health all influence how serious the event becomes.
In everyday life, the main takeaway is simple: a blood clot in lungs is a medical emergency, not a wait-and-see problem. Rapid care can be lifesaving.

Types Of blood clot in lungs
When people search for “blood clot in lungs,” they are usually asking about pulmonary embolism caused by a venous blood clot. That is the classic and most important form. Still, it helps to understand that doctors may think about it in a few practical ways.
Pulmonary embolism from a deep vein clot
This is the most common pattern. A clot forms in a deep vein, usually in the leg, then travels to the lungs and blocks a pulmonary artery or one of its branches. This is why leg swelling, warmth, redness, or calf pain sometimes show up before breathing symptoms. But it is also possible to have a pulmonary embolism without any clear DVT symptoms at all.
Large versus small pulmonary embolism
A large clot can block major blood flow and cause dramatic symptoms such as severe breathlessness, low blood pressure, fainting, or shock. Smaller clots may block smaller vessels and cause chest pain with breathing, a fast heart rate, cough, or reduced exercise tolerance. A person with underlying heart or lung disease may feel much worse from a clot size that another person might tolerate better.
Single versus multiple clots
Some people have one main clot. Others have several clots affecting different parts of the lungs. Multiple clots can reduce oxygen transfer more broadly and may make symptoms more persistent or recovery slower.
Rare non-blood blockages
Less commonly, blockages in lung vessels may involve material other than a typical blood clot, such as fat, tumor material, or air. These are not what most people mean when they say “blood clot in lungs,” but they help explain why the medical word “embolism” is broader than the everyday phrase.
Acute event versus longer-term consequences
The acute event is the immediate blockage. But some people continue to have lingering shortness of breath, reduced exercise capacity, or complications related to pressure in the lung circulation after the initial emergency has passed. Recovery is not always over in a few days. That is one reason follow-up matters.
Causes Of blood clot in lungs
A blood clot in lungs does not usually begin in the lungs themselves. The usual chain is this: a clot forms in a vein, part of it breaks off, and that moving piece gets stuck in the lung circulation. In practical terms, clots tend to form when blood flow becomes sluggish, a vein is injured, or the body becomes more prone to clotting than usual.
Slow blood flow
Blood moves best when muscles are helping pump it along and when a person is not sitting or lying still for long stretches. Long periods of immobility can slow circulation and give clots more opportunity to form.
Common real-life examples include:
- Recovery after surgery
- Hospital stays
- Prolonged bed rest due to illness or injury
- Wearing a leg cast
- Sitting for a long time during travel or desk work
Injury to a vein
Veins can be damaged by trauma, fractures, major surgery, or severe muscle injury. Once a vessel wall is irritated or injured, clotting becomes more likely. This is one reason the risk rises after operations involving the abdomen, pelvis, hips, or legs.
A body state that clots too easily
Some people have inherited clotting disorders. Others develop higher clot risk because of hormones, pregnancy, cancer, inflammation, or certain illnesses. Estrogen-containing birth control or hormone therapy can increase risk in some people. Pregnancy and the first few months after delivery also raise the chance of clot formation.
Cancer and serious medical conditions
Cancer and cancer treatment are strongly linked to clotting risk. So are some chronic illnesses, including heart disease, lung disease, and inflammatory bowel disease. Central venous catheters can also contribute in some patients.
Rare direct clots in lung vessels
In some cases, clotting can occur directly within the smaller blood vessels of the lungs, even when a clot in the arms or legs is not obvious. This is less typical, but it reminds us that pulmonary embolism is not always a simple one-step story.
The practical lesson is that pulmonary embolism often comes from a buildup of several ordinary risks rather than one dramatic trigger. A person may have recent travel, mild dehydration, hormone therapy, and a family history, for example. Each factor may seem manageable alone, but together they can shift the balance toward clotting.
Symptoms Of blood clot in lungs
The symptoms of a blood clot in lungs can range from subtle to sudden and terrifying. Some people feel sick within seconds or minutes. Others notice symptoms building over days or even weeks. That variation is one reason early recognition matters.
Common symptoms
The most common warning signs include:
- Sudden shortness of breath
- Chest pain or discomfort, especially pain that gets worse with a deep breath or coughing
- Fast breathing
- Fast or irregular heartbeat
- Cough
- Coughing up blood
- Lightheadedness or fainting
What symptoms may feel like in real life
A person may describe it as “I suddenly couldn’t get a full breath,” “my chest hurt when I inhaled,” or “I felt fine walking across the room yesterday, but today I get winded just climbing a few steps.” Some people feel anxious, sweaty, or shaky because the body senses a serious circulation problem. Others think they pulled a chest muscle because the pain is sharp and worse with breathing.
Signs that may point to a leg clot first
If the clot started in the leg, there may also be:
- Swelling in one leg or arm
- Pain or tenderness without an obvious injury
- Warm skin
- Redness or discoloration
Symptoms are not always complete or obvious
A very important detail is that you can have a pulmonary embolism without noticeable DVT symptoms. In other words, no swollen calf does not mean no lung clot. That is why unexplained chest pain or breathing trouble should not be ignored just because the legs look normal.
When symptoms suggest an emergency
Urgent care is especially important if symptoms are sudden, severe, or accompanied by fainting, very low blood pressure, marked weakness, or coughing up blood. In severe cases, a pulmonary embolism can cause shock or death before the diagnosis is even made.
Risk Factors
Almost anyone can develop a blood clot, but risk rises when several factors stack together. That is why two people can take the same long flight and only one develops trouble. The issue is usually not one single exposure. It is the overall risk picture.
Major risk factors to know
- Previous DVT or pulmonary embolism
- Family history of blood clots
- Inherited clotting disorders
- Recent surgery
- Recent hospitalization
- Prolonged bed rest or limited movement
- Long-distance travel, especially over 4 hours
- Pregnancy and the postpartum period
- Estrogen-containing birth control or hormone therapy
- Cancer and cancer treatment
- Older age
- Overweight or obesity
- Central venous catheters
- Heart disease, lung disease, or inflammatory bowel disease
- Smoking or tobacco use may add to overall vascular risk
Travel risk in context
Long travel gets a lot of attention, but the risk is generally small for most healthy travelers. The concern becomes more meaningful when long travel combines with other risks such as recent surgery, active cancer, pregnancy, obesity, older age, or prior clot history. That is why two people can take the same eight-hour trip and have very different levels of danger.
Hospitalization is a major real-world trigger
One of the most important patterns is healthcare-associated clotting. People who are currently hospitalized, recently discharged, or recovering from surgery may be at especially high risk. Many serious clots do not happen during the hospital stay itself. They happen after discharge, when people assume the danger has already passed.
Diagnosis Process
A blood clot in lungs cannot be diagnosed reliably from symptoms alone. That is because pulmonary embolism can look like pneumonia, a heart attack, anxiety, or other urgent conditions. Doctors usually combine symptoms, exam findings, risk factors, blood tests, and imaging to decide quickly what is going on.
Step 1: Urgent clinical assessment
The first step is often a fast review of symptoms, vital signs, oxygen levels, and recent history. A clinician may ask about surgery, travel, pregnancy, cancer, leg swelling, previous clots, medications, or whether symptoms came on suddenly. They may also examine the legs for swelling, tenderness, warmth, or redness.
Step 2: Blood testing
A D-dimer blood test may be used as an early screening step in some people, especially when the overall suspicion is not extremely high. A negative result can help rule out a clot in the right situation. Oxygen levels may also be checked, because low oxygen can support concern for a lung blockage, though normal oxygen does not completely rule one out.
Step 3: Imaging
The main imaging test for pulmonary embolism is CT pulmonary angiography, often called CTPA. This creates detailed images of the blood vessels in the lungs and is considered the standard imaging test for diagnosis. If CT is not appropriate or not definitive, a ventilation-perfusion scan, or V/Q scan, may be used to compare airflow and blood flow in the lungs.
Step 4: Looking for the source clot or strain on the body
Doctors may also use ultrasound to look for a clot in the leg veins or other tests to assess heart and lung function if needed. In selected cases, pulmonary angiography may be used when the diagnosis remains uncertain after other testing.
The key point for readers is simple: do not try to self-diagnose or “rule it out” at home. A blood clot in lungs is one of those conditions where imaging and medical evaluation matter.
Living With blood clot in lungs
Living with a blood clot in lungs usually means living through two phases: the emergency phase and the recovery phase. Many people focus only on surviving the acute event, but daily life afterward can still be challenging.
Treatment is often centered on blood thinners
The most common treatment is anticoagulation, often called blood-thinner treatment. These medicines do not magically erase the clot overnight. Their main job is to keep the clot from getting bigger and reduce the chance of new clots forming while the body gradually breaks down what is already there. Severe cases may require hospital care, clot-dissolving medicines, catheter-based treatment, surgery, or a vena cava filter if blood thinners cannot be used in the usual way.
Recovery may take longer than people expect
Some people feel noticeably better within days. Others need weeks or longer before their breathing and stamina improve. A pulmonary embolism can take months, and sometimes years, to fully resolve. That does not mean recovery is failing. It means healing can be gradual, especially if the clot was large or the person had other heart or lung issues to begin with.
Daily life after diagnosis
Common real-life issues include:
- Fatigue after mild activity
- Fear that every chest sensation means a new clot
- Worry about bleeding while taking blood thinners
- Disrupted routines due to follow-up visits and testing
- Reduced confidence with exercise or travel
- Anxiety about recurrence
Practical self-care habits that may help
- Take anticoagulants exactly as prescribed
- Do not stop treatment early without medical guidance
- Keep follow-up appointments and lab monitoring when required
- Return gradually to activity as advised
- Learn the warning signs of both another clot and serious bleeding
- Keep an updated medication list
- Ask for help if anxiety, fear, or sleep disruption becomes persistent
Longer-term complications to know about
Some people continue to have reduced exercise tolerance or ongoing symptoms after a pulmonary embolism. In recurrent or complicated cases, long-term pressure problems in the lung circulation can develop. Persistent or worsening shortness of breath after the acute event should not be brushed off as “just recovery” without follow-up.
Prevention Strategies
Prevention is often about reducing clot risk before a clot forms, not trying to guess when trouble will happen. The best strategy depends on the situation.
After surgery, injury, or hospitalization
Move as soon as it is medically safe. Ask whether preventive anticoagulants or compression stockings are appropriate. Know that the risk may continue after discharge, so it is worth understanding symptoms before going home.
During long travel
For trips longer than four hours by air, car, or bus, movement matters. Stand up or walk when possible. On flights, an aisle seat can make that easier. If you must stay seated, flex your feet, raise your heels and toes, and move your calves regularly. Travel risk is generally low for most people, but it rises when combined with other clot risks.
For people with known risk factors
If you have had a prior clot, have active cancer, are pregnant or recently postpartum, take estrogen therapy, or have a family history of clotting disorders, it is worth discussing prevention plans before surgery, long travel, or prolonged immobilization. Prevention may involve medicine, compression, earlier mobility, or a specific monitoring plan.
Everyday habits that support lower risk
- Stay physically active
- Avoid staying still for long stretches
- Maintain hydration, especially during travel or illness
- Avoid tobacco products
- Work toward a weight that supports overall health
- Do not ignore one-sided leg swelling or unexplained calf pain
Prevention does not guarantee a clot will never happen, but it can meaningfully lower risk, especially when applied during high-risk periods rather than only after symptoms begin.
Practical Examples
Example 1: The long-haul traveler
A 52-year-old office worker is taking a 10-hour flight. She also uses estrogen therapy and had knee surgery two months ago. Her risk is not the same as that of a healthy 25-year-old on the same plane.
A practical plan may include:
- Talk with her clinician before the trip
- Choose an aisle seat if possible
- Walk every 1 to 2 hours
- Do calf and ankle movements while seated
- Avoid spending the whole flight asleep in one position
- Know the symptoms that require immediate help after travel
Example 2: The recently discharged surgical patient
A man goes home three days after abdominal surgery. He assumes the danger is over because he is no longer in the hospital. But the recovery window after surgery is a classic time for blood clots.
A better routine looks like this:
- Follow discharge instructions on movement and medication
- Walk short distances regularly instead of staying in bed most of the day
- Ask whether compression stockings or preventive blood thinners are part of the plan
- Call promptly about leg swelling, chest pain, or sudden breathlessness
Example 3: The person recovering on blood thinners
A woman treated for pulmonary embolism is back home. Her biggest concerns are bleeding, recurrence, and exhaustion.
A realistic daily routine may include:
- Taking medicine at the same time each day
- Using a medication reminder
- Keeping follow-up appointments
- Increasing activity gradually rather than jumping back into intense exercise
- Avoiding activities that carry a high injury risk while anticoagulated
- Asking about mental health support if fear becomes overwhelming
Quick checklist: when a beginner should treat symptoms as urgent
Seek immediate medical attention for:
- Sudden shortness of breath
- Chest pain that gets worse with breathing
- Fainting or near fainting
- Coughing up blood
- Fast or irregular heartbeat with breathing difficulty
- New leg swelling plus chest symptoms
Do and don’t list
Do
- Move regularly during recovery and travel
- Learn your personal risk factors
- Take prescribed anticoagulants exactly as directed
- Keep follow-up care on schedule
Don’t
- Ignore sudden chest symptoms
- Assume no leg symptoms means no pulmonary embolism
- Stop blood thinners on your own
- Treat persistent post-PE shortness of breath as unimportant without checking in
Conclusion
A blood clot in lungs usually means pulmonary embolism, a potentially life-threatening blockage in the lung circulation that often begins as a clot in the deep veins of the leg. The most important things to remember are that symptoms can appear suddenly, diagnosis requires proper medical testing, and rapid treatment can make a major difference in survival and recovery.
In practical terms, people should know the emergency warning signs, understand their own risk factors, and take prevention seriously during high-risk times such as after surgery, during hospitalization, during long travel, and around pregnancy or cancer treatment. For those recovering from a pulmonary embolism, consistent treatment, follow-up, gradual return to activity, and attention to new symptoms are central parts of healing.
If there is one next step that matters most, it is this: do not downplay unexplained shortness of breath, chest pain with breathing, fainting, or coughing up blood. In the setting of a possible blood clot in lungs, timely evaluation matters.
Frequently Asked Questions
1. Is a blood clot in lungs the same as a pulmonary embolism?
Usually, yes. In everyday health content, “blood clot in lungs” usually means pulmonary embolism, which is a clot blocking blood flow in the lungs. Most often, that clot traveled from a deep vein in the leg.
2. Is a blood clot in lungs always an emergency?
Yes, it should be treated as urgent. Some pulmonary embolisms are smaller than others, but even a smaller clot can worsen or signal that more clots are present. Severe cases can become life-threatening very quickly.
3. Can you have a pulmonary embolism without leg pain?
Yes. A person can have a pulmonary embolism without obvious DVT symptoms in the leg. That is one reason the diagnosis can be missed if people wait for classic calf swelling first.
4. What does the chest pain usually feel like?
Many people describe it as sharp pain or discomfort that gets worse with a deep breath, coughing, or exertion. It does not always feel like the crushing pressure often associated with a heart attack.
5. Can a blood clot in lungs cause coughing up blood?
Yes. Coughing up blood can happen with pulmonary embolism and should be taken seriously, especially if it comes with chest pain or shortness of breath.
6. How do doctors confirm the diagnosis?
Doctors often use a combination of symptom review, risk assessment, blood testing such as D-dimer, oxygen checks, and imaging. CT pulmonary angiography is the standard imaging test for many patients, while a V/Q scan may be used in some situations.
7. How is a blood clot in lungs treated?
Treatment commonly involves anticoagulants, also called blood thinners. In severe or unstable cases, treatment may include clot-dissolving medicine, procedures to remove or break up the clot, or a vena cava filter for selected situations.
8. How long do people stay on blood thinners after a pulmonary embolism?
It depends on the individual reason for the clot, the risk of recurrence, and bleeding risk. Some people are treated for a few months, while others may need longer-term treatment. Follow-up with a qualified clinician is essential.
9. How long does recovery take?
Some people feel better within a week, but full recovery can take much longer. A pulmonary embolism may take months, and sometimes years, to completely resolve. Stamina often returns gradually rather than all at once.
10. Can a blood clot in lungs come back?
Yes. Recurrence is possible, especially if underlying risk factors remain or treatment is stopped too early. That is why ongoing care and prevention planning matter.
11. Are long flights dangerous for everyone?
Not necessarily. For most healthy travelers, the risk is generally small. The concern rises when long travel is combined with other factors such as recent surgery, previous clot history, cancer, pregnancy, estrogen use, obesity, or older age.
12. What are the signs of a DVT that might come before a pulmonary embolism?
Typical signs include swelling in one leg or arm, unexplained pain or tenderness, warmth, and redness or discoloration. These symptoms deserve prompt medical attention, especially if chest symptoms also appear.
13. Can a blood clot in lungs be prevented?
Sometimes, yes. Risk can often be reduced by moving early after surgery or illness, avoiding long periods of immobility, staying active during travel, and using prevention tools such as compression or medication when a clinician recommends them.
14. When should someone go to the emergency room instead of waiting for a clinic visit?
Emergency evaluation is appropriate for sudden shortness of breath, chest pain with breathing, fainting, coughing up blood, or a rapid heartbeat with breathing trouble. Those symptoms should not be monitored at home in hopes they will pass.
Final Editorial Disclaimer
This article is for educational purposes only and does not replace medical advice, diagnosis, or treatment from a qualified healthcare professional. A blood clot in lungs can be life-threatening and requires timely medical evaluation. Anyone with severe chest pain, sudden breathing difficulty, fainting, coughing up blood, or other serious symptoms should seek urgent medical care right away.